
Today's physical exam rounds were on clubbing. Some points:
Etiologies (not meant to be exhaustive!)
1) Pulmonary- neoplastic, suppurative (i.e. abscess, empyema), bronchiectasis, inflammatory (e.g. fibrosis), pulmonary AVMs (as in HHT)
2) Cardiac- cyanotic heart disease, endocarditis
3) GI- cirrhosis (often non-alcohol related, as in PBC), celiac, IBD
Others: alpha-1 antitrypsin deficiency, sarcoma, hyperthyroidism
Classically first appears on 4th finger on non-dominant hand
Physical examination for clubbing:
May see obvious changes of terminal phalanges
Nailfold angles
1) Profile angle (AKA Lovibond's angle): Between skin proximal to cuticle and "takeoff" of nail; should be less than 180 degrees
2) Hyponychial angle: between skin proximal to cuticle and distal nail; should be less than 192 degrees.
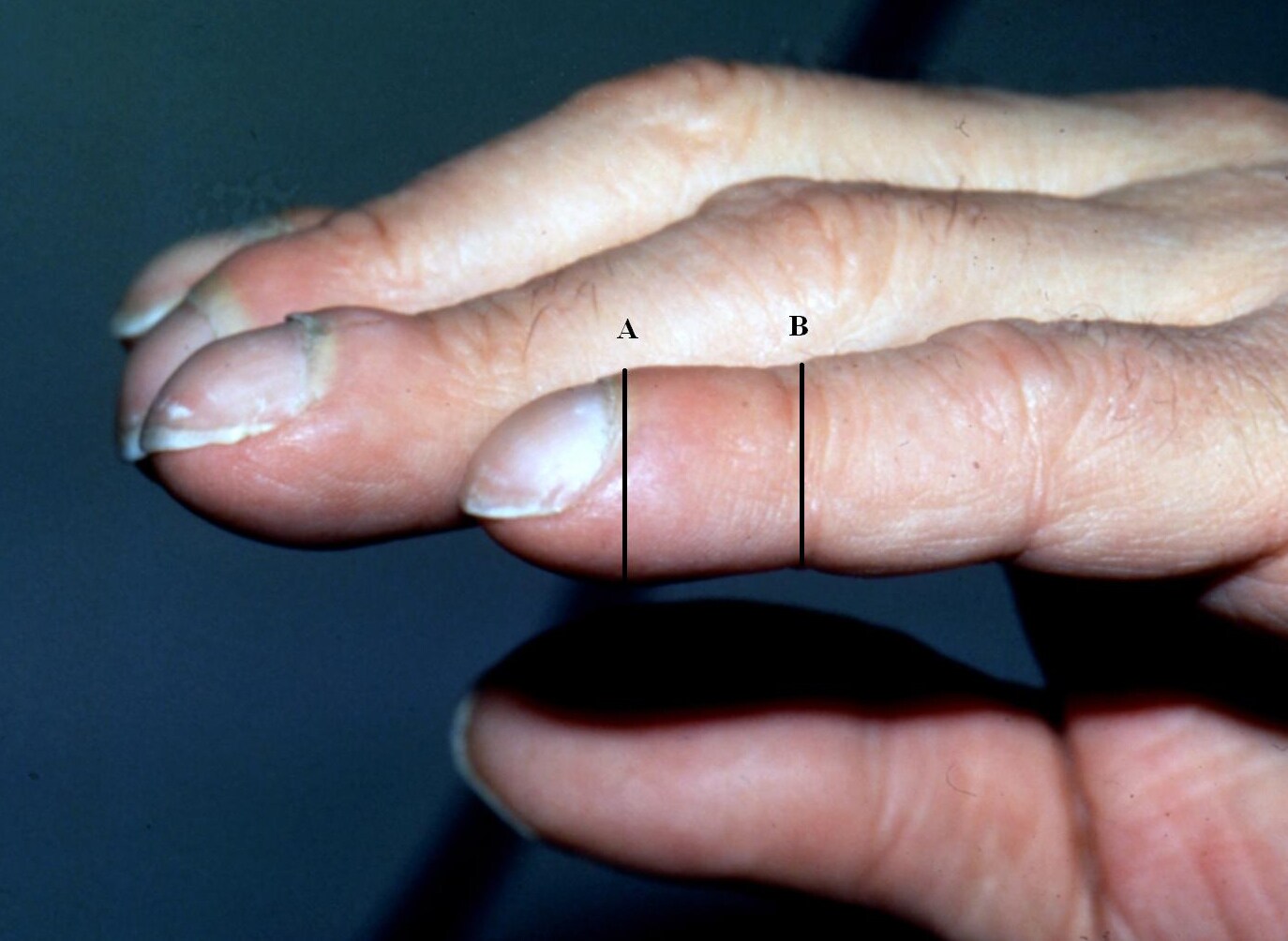
Phalangeal depth ratio
Ratio of the distal phalangeal depth (i.e. vertical height of the finger at the middle of the distal phanynx) to the interphalangeal depth (i.e. vertical height of the finger at the DIP joint). Interphanangeal depth is normally greater than distal phanangeal depth. This is reversed in clubbing.
Schamroth sign
Diamond-shaped opening when dorsal distal phalanges are opposed
Palpation:
May have "boggy" nailbed, where proximal edge of nail is felt, and may be able to rock the nail back and forth using nailbed as a fulcrum
Evidence:
Based on the JAMA Rational Clinical Exam article on clubbing,
the lack of an accepted gold standard makes sensitivity and specificty determinations difficult. Their literature review showed that 'normals' are very unlikely to have profile angle over 176 degrees, hyponychial angle over 192 degrees, or phalangeal depth ratio over 1.0. Patients are more likely to have IBD or lung cancer if clubbing is present, and the phalangeal depth ratio was the best test for this purpose.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}